Is surgery the best option or not, in the case of cancer in the head and neck? As the consequences for speaking and swallowing may be severe, some way of predicting these consequences would help in the decision-making. Performing surgery on a 3D virtual copy of the patient first, will give valuable information, says Technical Medicine PhD student Merijn Eskes of the University of Twente. He did his research in the Antoni van Leeuwenhoek hospital in Amsterdam.
Cancer in the head and neck area, like in the mouth cavity, throat or larynx, is in the top five of cancer types occurring most often. In many cases, the tumor is discovered in a late stage, causing a poor prognosis and limited treatment options. Operative removal of the tumor is not always possiblen, as other vital functions may be affected. In other cases, an operation is possible, but for other reasons not desirable: it will take place at the most visible part of the body and seriously affects the way a patient looks, speaks, chews and swallows. The patient can’t imagine how he or she will look after the operation. One surgeon chooses for an operation easier than the other. If the surgeons would have a virtual version of the patient, built up from scans and measurements, they can perform a virtual operation, see the consequences and discuss them with the patient.

In order to develop a ‘digital ‘ of the patient, Merijn Eskes had studied the muscle control in the face. An Electromyogram (EMG) gives information on the muscles and neural control. This is done by placing electrodes on the face, just like the electrodes that are placed on the skull in the case of EEG. By measuring the signals of 16 facial muscles, Eskes is capable of predicting lip movements. He prefers biomechanical models for this: they give better results than models that are merely statistical. Combining the EMG data with the results from X-Ray, MRI and CT, the basics of the ‘virtual patient’ can be built.
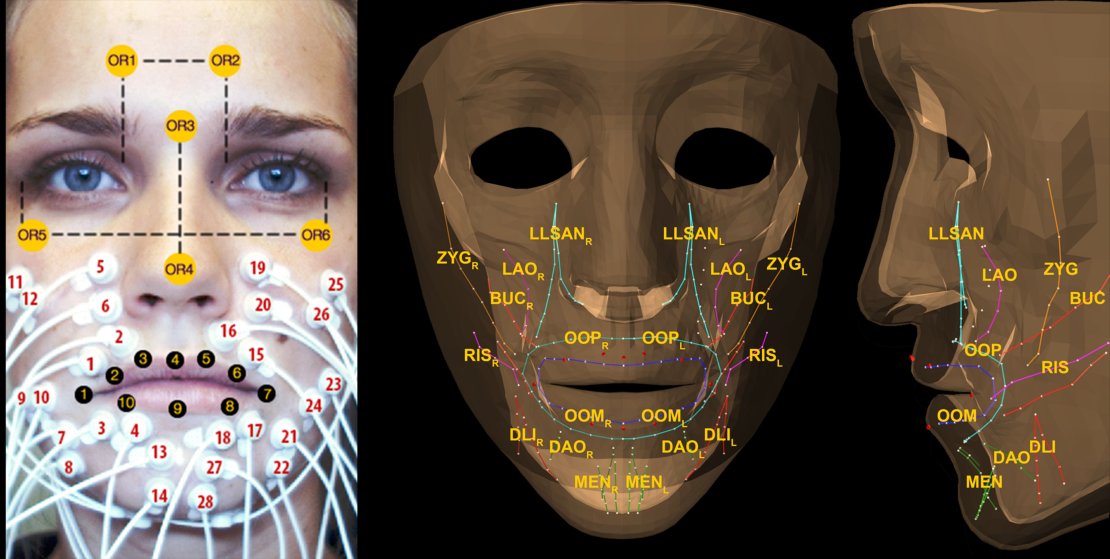
A test subject wearing 16 EMG electrodes for measuring muscle activities and lip markers to capture the movements using a 3D camera. On the right: the biomechanical model in ‘ArtiSynth’ (www.artisynth.org) used by Eskes. The abbreviations of the muscle names: ZYG, zygomaticus major, RIS, risorius, LLSAN levator labii superioris aleque nasi, LAO levator anguli oris, BUC buccinators, OOP Orbicularis oris peripheralis, OOM, marginalis, DLI depressor labii inferior DAO depressor anguli oris and MEN mentalis
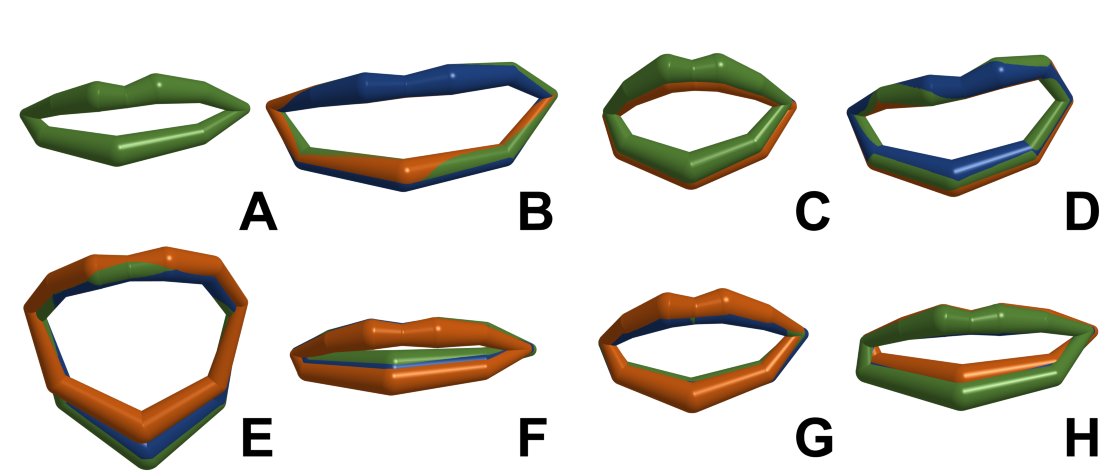
Measured 3D shape of the lips for various facial expressions, in green. The blue and orange 3D lip shapes were predicted using two different statistical models based on muscle activation signals using EMG. A. rest B. voluntary smile, C pursed lips, E mouth open, F depressed mouth corners, G blowing H pouting.
Learned strategies
What complicates things, is that patients behave differently. One patient, for example, will develop compensation strategies without any training, compensating for the lost functionality using other muscles. Another patient doesn’t succeed in this at all, even after a lot of training. By using ‘inverse modelling’, you could use the values you measure now for reconstructing the patterns that a patient learned during his life. In general, this gives far too many solutions. But using the EMG data, this amount of possible solutions is strongly reduced. A truly patient specific model comes closer.
Eskes’ research is part of a larger ‘Virtual Therapy’ project of the Head and Neck Oncology and Surgery Center of the Antoni van Leeuwenhoek hospital. Previous projects, also by Technical Medicine students and PhD’s of the University of Twente, looked at 3D modeling of the tongue, for example. Eskes’ new results are an important step towards a virtual patient. It will take about five years before there is a model that can be used in clinical practice, he predicts.
Personalized healthcare
The PhD research fits well within one of the recenty defined research themes of the University of Twente: 'Improving healthcare by personalized technologies'. Students and PhD's of the Technical Medicine programme, like Eskes, play a major role in introducing technology into healthcare.
Merijn Eskes (Winterswijk, 1987) studied Technical Medicine at the University of Twente. On 13 december he defends his thesis ‘Surface electromyography in personalised modelling of the head and neck’. His promotors are Prof. Kees Slump (UT) en Prof. Fons Balm (AvL). Dr. Ferdi van der Heijden was his daily supervisor.




