Twents Onderzoek naar Recidieven na Bekkenbodem Operaties
PROJECT ACRONYM
TORBO
FUNDED BY
ZGT Wetenschapsvoucher
PHD CANDIDATE
Graduate student (M3) Technical Medicine Inge Rikkers
Rotating M2 Technical Medicine students
SUPERVISORS
Gynecologists: Annemarie van der Steen / Angelique Veenstra van Nieuwenhoven
UT: Frank Simonis / Anique Bellos-Grob
COLLABORATION
Ziekenhuisgroep Twente (ZGT)
CLINICAL BACKGROUND
Pelvic organ prolapse (POP) is characterized by a pelvic floor organ (e.g. bladder, uterus, bowel) protruding (prolapsing) from the opening of the vagina. The main treatment options for POP are conservative treatment with a pessary or surgical correction. In the Netherlands, the prevalence of symptomatic POP in women between 45-85 years is 11.4% and the average number of women who receive surgery based on complaints of POP or urinary/fecal incontinence are as high as 10-20%. Multiple (combinations of) POP are defined, based on the prolapsed organ: anterior, apical and posterior compartment prolapse. Based on the physical complaints, recurrence surgery and the prolapsed compartment(s) the best surgical treatment option is selected. The different options are: anterior/posterior colporrhaphy, sacrospinal fixation (SSF), (modified) Manchester Fothergill (MF), rectopexy, sacrocolpopexy (SCP) and vaginal hysterectomy (VH). Surgical correction has turned out to be highly effective, however the estimated risk of reoperation over a period of 4 years is 30%, while reasons for recurrences are poorly understood. At the University of Twente (UT) we have the unique possibility of visualizing the pelvic floor, and pelvic organ prolapse in upright position. We hypothesize that recurrences and continuation of physical complaints might be related to the pre-operative and post-operative (incomplete) assessment of the prolapse (POP-Q) in supine position. Crucial anatomical details, related to surgical treatment and success are missed or underdiagnosed.
OBJECTIVE
Investigate the effect of surgery on the position and shape of the pelvic organs, the functionality of the pelvic floor muscles and it relation to recurrences and differences in the assessment of prolapse recurrences in supine and upright position.
PROJECT DETAILS
TORBO is executed in a multi-phase set-up. All steps include:
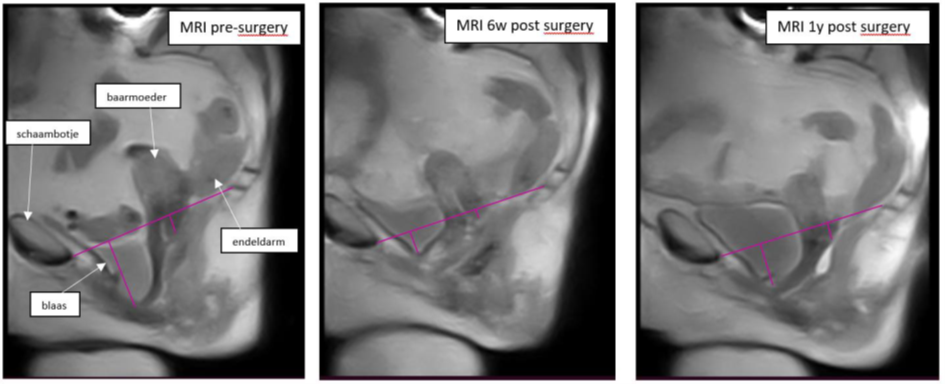
1. MRI scans in supine and upright position
2. Transperineal ultrasound scans
3. Questionnaire on disease specific conditions and quality of life
Phase 1: A total of 65 POP-patients, scheduled for at least anterior colphorrage will be included. Patients will be scanned before surgery and 6 weeks, 1 year and 2 years after surgery. Inclusion started in April 2022.
Phase 1B: A total of 15 POP-patients, scheduled for at least rectopexy surgery will be included. Patients will be scanned before surgery and at 6 weeks after surgery.
Grob ATM, Olde Heuvel J, Futterer JJ, Massop D, Veenstra van Nieuwenhoven AL, Simonis FFJ, van der Vaart CH. Underestimation of pelvic organ prolapse in the supine straining position, based on magnetic resonance imaging findings. Int Urogynecol J. 2019 Nov;30(11):1939-1944. doi: 10.1007/s00192-018-03862-0. Epub 2019 Jan 17. PMID: 30656361; PMCID: PMC6834735.