In vivo blood flow quantification with echoPIV
Introduction
Imaging of endovascular flow patterns in the abdominal aorta is challenging, due to the anatomical position of these arteries and flow velocities ranging between 1 m/s and backward flow during diastole. Assessment of these local flow patterns is clinically relevant as flow abnormalities have been related to atherosclerotic disease progression and patency loss of stents placed in the aorto-iliac tract.
Improved quantification and understanding of these mechanisms can lead to improved pre-procedural planning and follow-up in endovascular treatment of the aorto-iliac tract. To achieve this, it is important to obtain a reliable method for the quantification of blood flow in the abdomen.
Ultrasound particle image velocimetry (echoPIV) has been used to quantify two-dimensional blood flow within a limited range of velocities, on a small number of subjects. In this technique, high frame rate, contrast-enhanced ultrasound (HFR-CEUS) images are acquired and used for particle image velocimetry (PIV) analysis to obtain velocity vector fields of blood flow.
Completed project: volunteer study
A study was recently executed in collaboration with the Erasmus MC to assess the feasibility of echoPIV in the abdominal aorta and to compare the technique to phase contrast magnetic resonance imaging (PC-MRI).
Methods
14 healthy volunteers (age 18 to 35 and BMI < 25) received multiple HFR-CEUS scans using a Verasonics Ultrasound machine. Several ultrasound contrast agent (UCA) dosages and Mechanical Index (MI) values were compared. PIV analysis was performed through pairwise cross-correlation of all captured images. Volunteers also underwent PC-MRI. Comparison of the echoPIV and PC-MRI velocity profiles was performed by calculation of similarity index (SI) and relative difference in peak velocity (difpeak).
Results
Visualization of the aortic bifurcation using HFR-CEUS was successful in all volunteers. Optimal echoPIV results were achieved with the lowest UCA dosage in combination with the lowest MI. Significant bubble destruction occurred at higher MI. Similar flow patterns could be observed in both the echoPIV and PC-MRI data and velocity profiles showed good agreement (fig 1 left and right). Video 1 shows the full vector field during 1 cardiac cycle.
Conclusion
Quantification of blood flow in the abdominal aorta with echoPIV was proven to be feasible, for the first time in humans. The echoPIV technique potentially has a high clinical value in diagnosis and follow-up of arterial diseases.
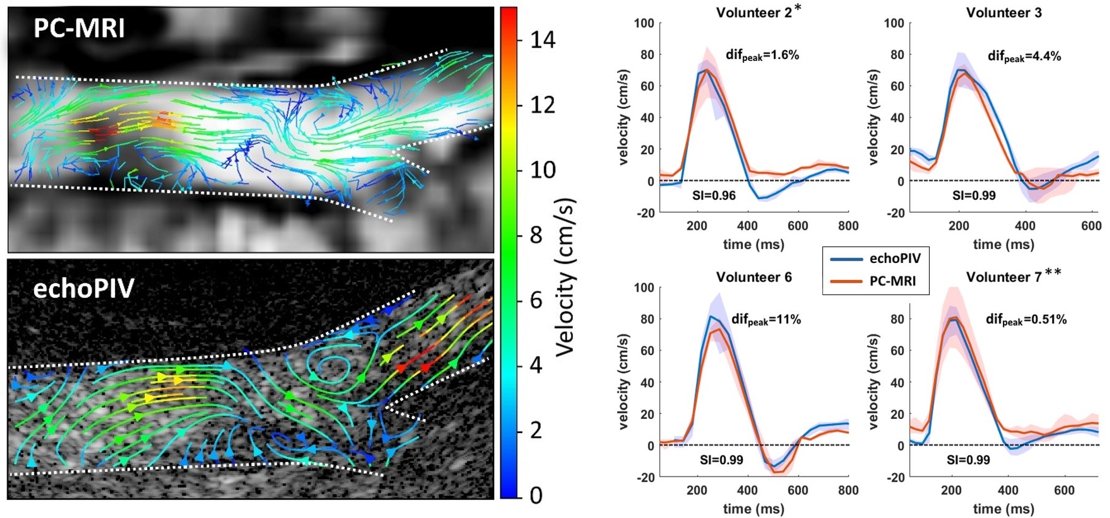
Figure 1. Left, streamline representation of blood flow velocities during early diastole in volunteer 7. Similar flow patterns can be observed in both datasets. Right: temporal velocity profiles in 4 volunteers. Difpeak = relative difference in peak velocity, relative to PC-MRI data. SI = Similarity Index.
Video1. Processed in vivo echoPIV recording obtained at the aortic bifurcation.
Current project: patient studies
In this project a large clinical study will be executed in the Rijnstate hospital. In this study echoPIV will be used to identify local flow patterns that can predict disease progression and failure of stent patency in patients with untreated and treated atherosclerotic lesions in the aortoiliac tract.
Study design
Prospective cohort study. Subjects will receive ultrasound particle image velocimetry (echoPIV) measurements at baseline to obtain blood flow velocity data and to calculate flow derived parameters, such as: mean wall shear stress (WSS), oscillatory shear index (OSI), recirculation and blood stasis. 2 year follow-up of subjects will be performed to measure clinical outcome parameters, such as lesion severity, walking distance and stent patency. The influence of the calculated flow parameters on these outcome parameters will be investigated.
Study population
The study population consists of three different patient groups. Group A: 70 patients with a recently diagnosed stenotic lesion in the iliac arteries, with intermittent claudication, that are treated with exercise therapy. Group B: 40 patients that receive endovascular treatment (single stent placement) of an isolated iliac stenotic lesion. Group C: 20 patients that receive endovascular treatment of extensive aortoiliac stenotic lesions with covered endovascular reconstruction of the aortic bifurcation (CERAB).
Contacts


