Background
Chronic liver inflammation results in fibrotic changes of liver parenchyma in a large proportion of patients. The stage of advanced liver fibrosis is called liver cirrhosis, and it is in this stage that patients face complications of their chronic liver disease. These complications are associated with increased pressure in the portal system of the abdomen (portal hypertension) which results into development of free fluid in the abdomen (ascites), spontaneous bleeds of GI tract, and several clinical complications due to liver failure. 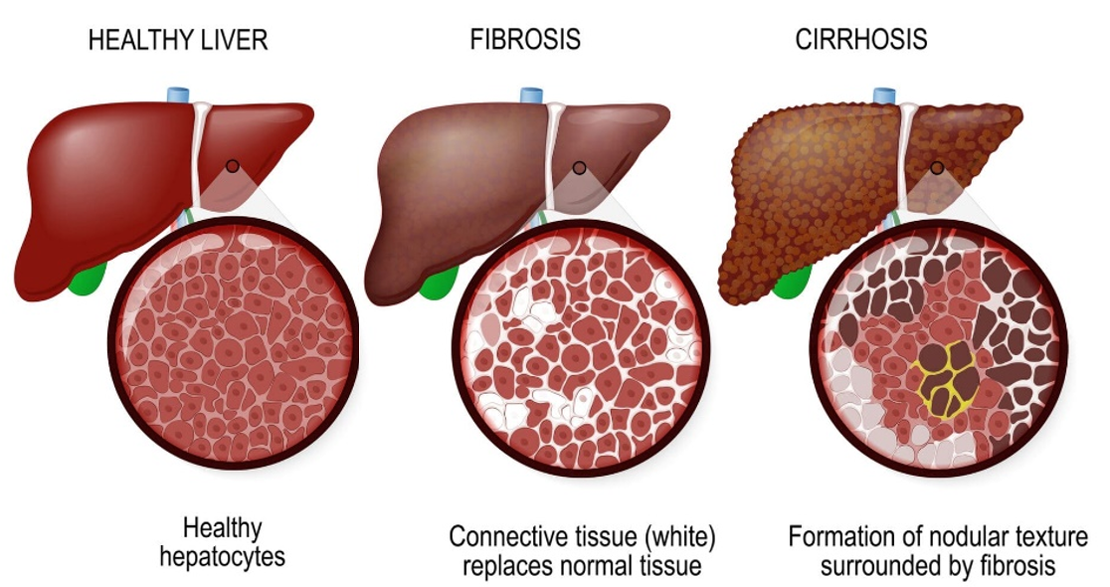
Figure 1 : Development of liver cirrhosis. Chronic inflammation results into development of fibrotic strands, resulting into a nodular structure of the liver.
Development of spontaneous bacterial peritonitis (SBP): Patients with portal hypertension often experience changes in the intestinal mucosa, commonly referred to as a 'leaky gut,' which leads to the translocation of bacteria from the intestinal lumen into the free abdominal cavity (figure 2, depicted at 1). In case of liver cirrhosis, the free abdominal cavity is filled with fluid (ascites) which provides an excellent environment for growth of bacteria resulting into SBP. SBP in a serious medical condition as its clinical presentation is atypical whereas it can soon develop towards sepsis and multi-organ failure with high mortality rates. It is for this reason that clinical guidelines recommend routine assessment for SBP for all patients with liver cirrhosis and clinical deteriorations. The current testing requires ascitic fluid testing by laboratories on presence of neutrophils. 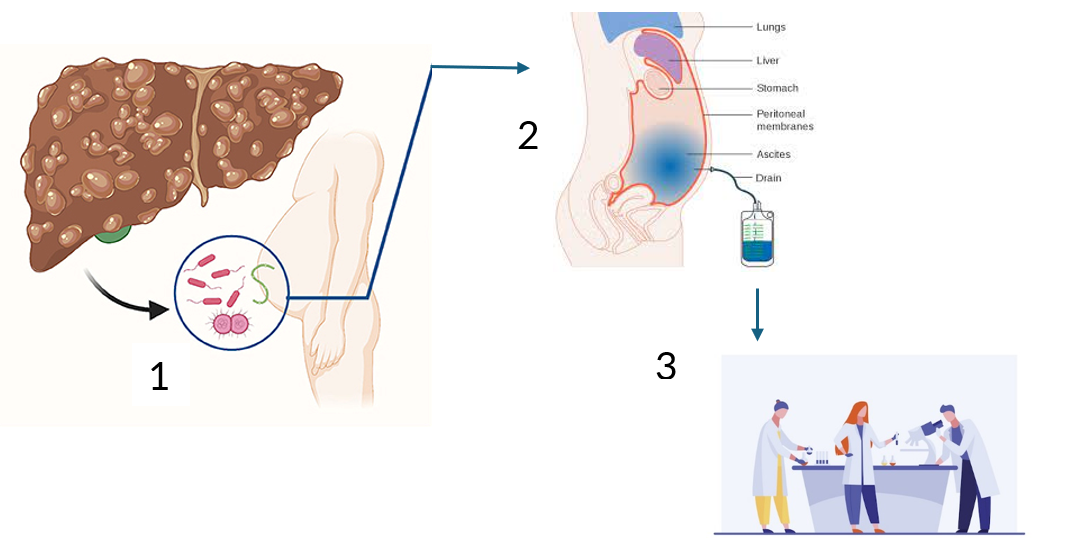
Figure 2: Current testing for SBP. Translocation of bacteria from the gut into ascitic fluids in case of liver cirrhosis results in SBP (1), Diagnosis of SBP requires an ascitic tap (2), which is tested for the presence of neutrophils by laboratory (3)
Current problem
Samples are sent to clinical chemistry for a standard cell count and differentiation using an automated analyzer. However, additional ascitic cells (e.g., mesenchymal cells) often require manual differentiation, which is time-consuming and can take hours or overnight, which contributes to severe delays, especially during off-hours. Delays in diagnosis and treatment are associated with longer intensive care and hospital stays, as well as increased mortality. The laboratory delays often lead to a presumed diagnosis at hospital admission, without clear confirmation. This results in empirical antibiotic use, contributing to unnecessary prescriptions and antibiotic resistance.
Solution
Lab-on-a-chip provides several opportunities to facilitate rapid diagnosis of SBP. The current project involves the first steps in the development of a bed-side lab-on-chip diagnostic tool (SPOT device) which would replace laboratory assessment.
The impact of the project is relevant at multiple levels; 1) Patients will benefit from a fast diagnosis and rapid initiation of treatment, reducing mortality rates; 2) A rapid diagnosis will avoid empirical and unnecessary usage of antibiotics, 3) A bed-side test reduces the burden on laboratory work load.

Figure 3 : The envisioned SPOT device
Assignment
In this assignment you will develop and test a lab-on-a-chip device able to count neutrophils in ascitic fluid. This diagnostic chip will consist of two areas (figure 3). First, a micropillar array with specific antibodies to deplete lymphocytes from the fluid. Second, an area for neutrophil counting using electrical impedance, featuring a 20-40 µm microchannel and planar electrodes.